
Tumors | Bone tumors | Osteoid Osteoma (cortical) od the Hip Socket (CT Scan and MRI)
24 year old patient adressed for cartilagineous and labral investigation due to left hip pain.
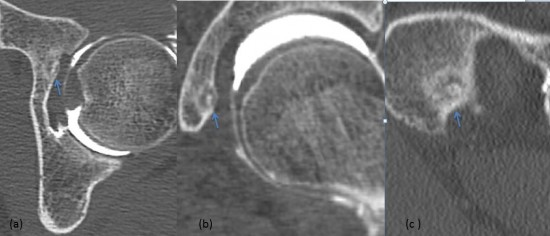
Arthro CT of the left hip :
Images (a) axial slice, (b) coronal slice and (c) sagittal slice : Centimetric lacunar image of the anterior aspect of the left hip socket with a central calcification (blue arrow). It is accompanied by a peripheric condensation progressively degressive to the normal bone, suggestive of an inflammatory lacuna.
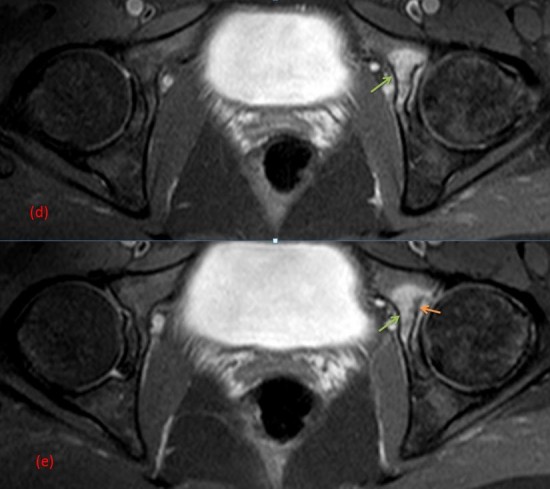
MRI of the hips :
Images (d) and (e) : DP SPIR weighted axial slices : Inflammatory high signal intensity of the left hip socket (green arrow) surrounding a small cortical image presenting in hyposignal (orange arrow).
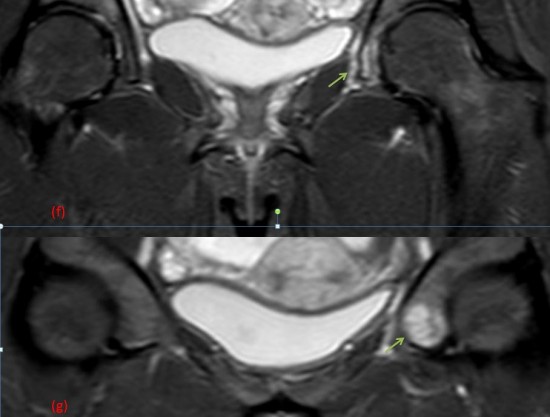
Images (f) et (g) : DP SPIR weighted coronal slices: Inflammatory high signal intensity of the left hip socket extensive to the surrounding soft tissue (green arrow)
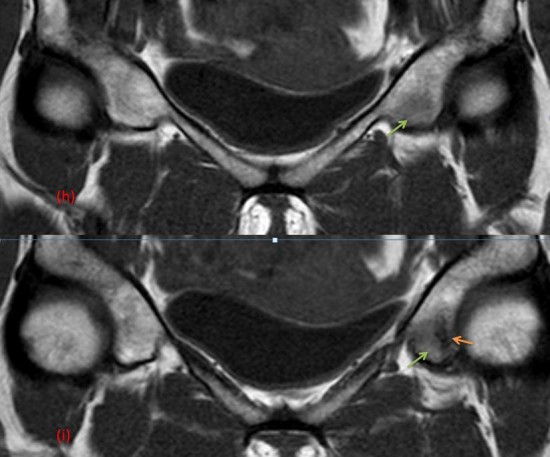
Images (h) et (i) : T1 weighted slices : Moderate low signal intensity of the left hip socket in keeping with an inflammatory edema (green arrow) surrounding a small cortical markedly low signal intensity region (orange arrow).
This case illustrates an osteoid osteoma of the left hip socket, which explains the patient's pain.
It is a relatively frequent benign tumor (15% of benign tumors) of the young person (5-30 years old). Clinical symptoms are nightly painful peaks calmed by the intake of aspirin. It affects most frequently long bones (femur and tibia) but also the spine and flat bones. Is of classical diaphysal and cortical topography.
On the therapeutic side, percutaneous treatment can be considered firstly(radiofrequency, laser photocoagulation, alcoholisation and percutaneous exeresis). Surgical treatment is the second choice, because it is more invasive.
J Med Case Rep. 2016 Aug 24;10(1):232. doi: 10.1186/s13256-016-1016-2.
J Med Case Rep. 2016 Dec 3;10(1):348.
