
Foot | Bone pathology | Osteitis of the Diabetic Foot
50 year old type 2 diabetic patient, with history of trans metatarsal amputation, presenting with a red hot foot in a contexte of back foot wound. MRI Scan.
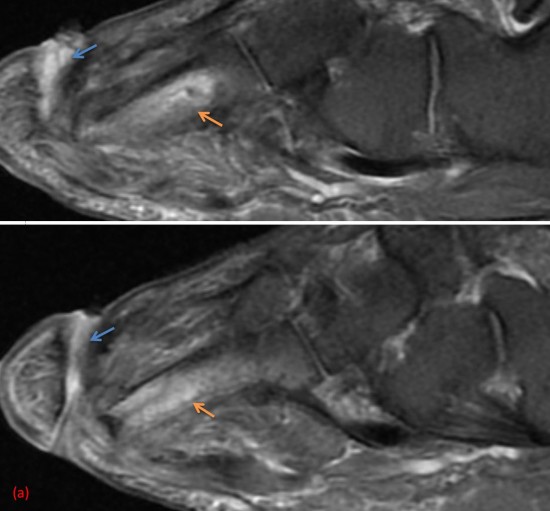
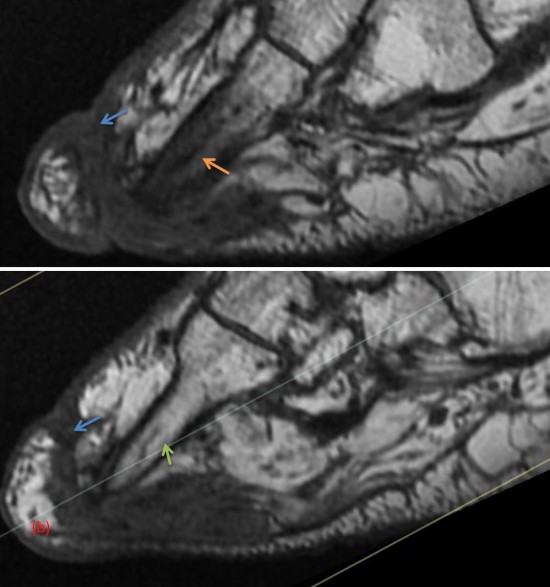
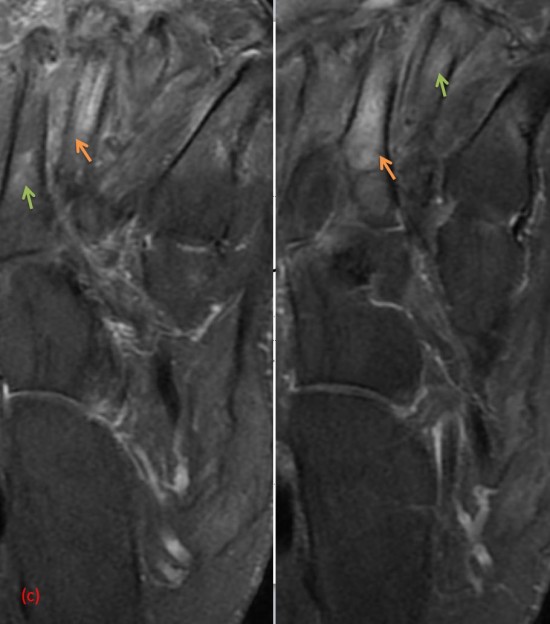
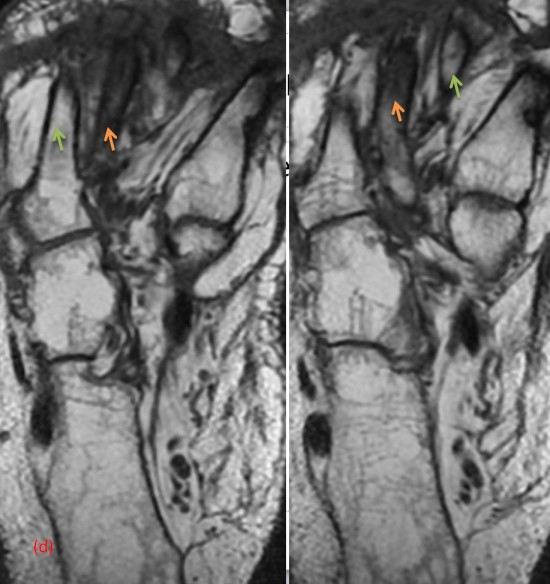
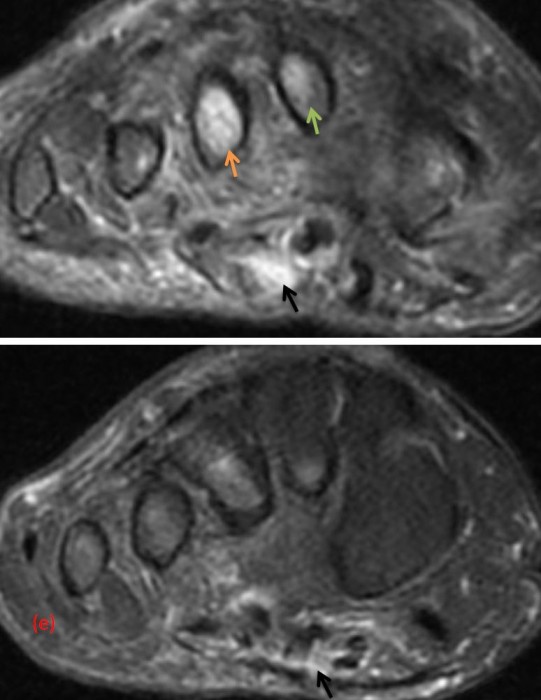
Image (a) : Sagittal DP FAT SAT weighted slices of the front foot : Cutaneous ulceration of the back side of the foot with drainage sinus (blue arrow), presenting in high intensity signal, adjacent to the 3rd metatarsal diaphysis. Association of high intensity signal of the spongy bone of the 3rd metatarsus (orange arrow).
Image (b) : Corresponding sagittal T1 weighted slices : the drainage sinus (blue arrow) appears in hyposignal. Association with a marked hyposignal of the spongy bone of the 3rd metatarsus (orange arrow), in keeping with a bone marrow oedema, evoking an osteitis. Note the respect of the spongy bone of the 2nd metatarsus (green arrow).
Image (c) : Corresponding axial DP FAT SAT weighted slices : high intensity signal (bone marrow oedema) of the 3rd metatarsus (orange arrow). Subtle high intensity signal of the 2nd and 4th metatarsi. (green arrows)
Image (d) : Axial T1 weighted slices : marked low intensity signal (osteitis) of the 3rd metatarsus (orange a rrow). No corresponding anomalies on the T1 slices, of the high intensity signal of the 2nd and 4th metatarsi visible on the DP FAT SAT slices, in keeping with simple wrong foot positioning. (green arrows)
Image (e) : Coronal DP FAT SAT weighted slices : liquid infiltration of the surrounding soft tissue with inter tendinous predominance, not compatible with an abcess on this non injected examination (black arrows). 3rd metatarsus osteitis (orange arrow).
Conclusion :
This case illustrates a 3rd metatarsus osteitis of the diabetic foot secondary to a foot wound.
Infection is most frequent in diabetic patients due to dysfunctional phagocytar cells. It is essentially bacterial or fungal and more severe than in non diabetic patients.
These infections can be secondary to cutaneous ulcers, which are favored by peripheral neuropathy, foot deformations and arteriopathy.
The differential diagnosis is nervous osteoarthropathy but the signs mostly in favour of the latter are : preferential involvment of the Chopart and Lisfranc, articular involvment with sub chondral damage, poly articular damage, moderately low intensity signal of the bone oedema and absence of cutaneous ulcer.
Imagerie musculosquelettique, pathologies générales, Cotten
Gil HC, Morrison WB. MR Imaging of diabetic foot infection. Semin Musculoskelet Radiol 2004;8:189-98.
